
 Fact-checked by
Fact-checked by 
Soliris (eculizumab) for neuromyelitis optica
What is Soliris for neuromyelitis optica?
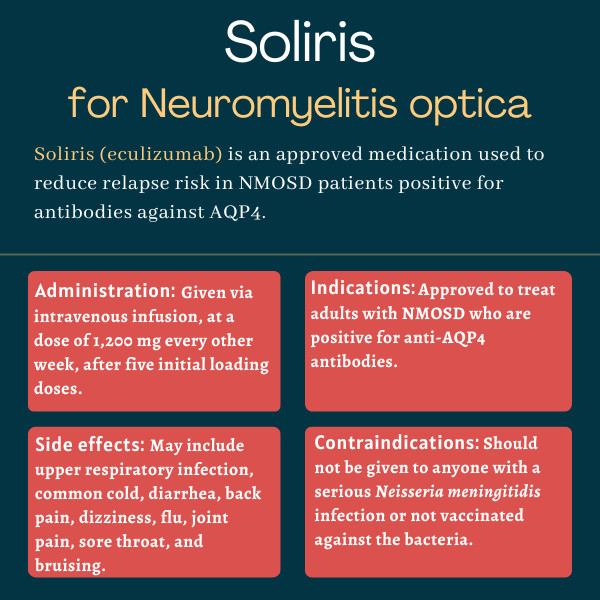
Soliris (eculizumab) is an infusion therapy approved to treat adults with neuromyelitis optica spectrum disorder (NMOSD) who are positive for antibodies against the aquaporin-4 (AQP4) protein — the most common target of self-reactive antibodies in NMOSD.
Administered as an into-the-vein, or intravenous, infusion, it works to reduce the risk of relapses for people with the autoimmune disease by modulating the body’s immune response. It was the first therapy approved in the U.S. for treating NMOSD.
Originally developed by Alexion Pharmaceuticals (now known as Alexion, AstraZeneca Rare Disease), Soliris also is approved for conditions sharing some of NMOSD’s underlying immune-related mechanisms. These disorders include paroxysmal nocturnal hemoglobinuria, or PHN, atypical hemolytic uremic syndrome, known as aHUS, and generalized myasthenia gravis, called gMG.
Therapy Snapshot
| Brand name: | Soliris |
| Chemical name: | Eculizumab |
| Usage: | Used to reduce relapses in neuromyelitis optica spectrum disorder |
| Administration: | Intravenous infusion |
How does Soliris work?
NMOSD is a rare autoimmune disease in which the immune system mistakenly attacks healthy parts of the nervous system, most commonly the spinal cord and the optic nerve, which relays signals between the eyes and the brain.
This autoimmune attack is typically driven by self-reactive antibodies against AQP4, a protein found at the surface of nerve-supporting cells called astrocytes. The binding of these antibodies to AQP4 activates the immune system’s complement pathway, comprised of circulating proteins that are typically in an inactive state.
Complement activation leads to a chain reaction that promotes inflammation and the formation of the membrane attack complex (MAC), a group of complement proteins that form holes in the membrane of cells, causing them to burst and die.
MAC formation is dependent on the cleavage of complement factor 5 (C5) into two subunits: C5a and C5b. An antibody-based therapy, Soliris works by binding to C5 and preventing that cleavage. That, in turn, suppresses MAC formation and the cell death it induces.
The therapy is thus expected to reduce the autoimmune damage that drives NMOSD, ultimately reducing disease activity and relapses.
Soliris is the predecessor of Alexion’s Ultomiris (ravulizumab-cwvz), a therapy subsequently approved for NMOSD with essentially the same mechanism of action but slightly modified to last longer in the body, thereby allowing for less frequent dosing.
Who can take Soliris?
Soliris was approved by the U.S. Food and Drug Administration in 2019 for the treatment of adults with NMOSD who are positive for anti-AQP4 antibodies. The decision made Soliris the first therapy to be approved in the country for the rare autoimmune disease.
In Canada and Japan, the therapy is available for the same indication. In the European Union, where the therapy’s approval followed that of the U.S. by two months, also in 2019, eligible patients must also have a relapsing disease course.
Because Soliris can increase a the risk of potentially life-threatening meningococcal infections — those caused by the Neisseria meningitidis bacterium — the medication is available in the U.S. only through a restricted access program.
Called Soliris REMS (Risk Evaluation and Mitigation Strategy), the program ensures that only certified healthcare professionals can prescribe Soliris and that both physicians and patients are fully informed about this risk and equipped to respond effectively if any signs of such infections become apparent. The program also ensures that all possible preventive measures are implemented prior to the start of Soliris treatment.
Who should not take Soliris?
The prescribing label for Soliris has a boxed warning for serious, life-threatening meningococcal infections, as these have occurred in patients treated with the medication and some have been fatal
For this reason, the medication is not recommended for anyone with an unresolved serious Neisseria meningitidis infection.
Soliris also should not be used in patients who are not up to date with vaccination against this bacterium, unless the risks of delaying treatment outweigh the potential risk of a serious meningococcal infection. In such cases, patients should receive preventive antibiotic treatment before starting Soliris.
How is Soliris administered in neuromyelitis optica?
Soliris is administered through infusions into the bloodstream at a recommended dose of 1,200 mg, given every two weeks.
First, however, five infusions, called loading doses, are given once weekly — the first four at a dose of 900 mg, and the fifth at a dose of 1,200 mg.
Subsequent infusions, called maintenance doses, are administered every other week at a dose of 1,200 mg. Patients should receive the therapy at these time points, or within two days of them.
Those also receiving treatment with plasma exchange, a blood-cleaning procedure that can decrease Soliris circulating levels, or fresh frozen plasma may need supplemental doses of the medication.
Soliris infusions usually take 35 minutes, but may last up to two hours if patients experience adverse reactions during administration and the infusion speed is subsequently slowed. Patients also should be monitored for at least one hour after the infusion for signs or symptoms of infusion-related reactions.
Soliris in clinical trials
Soliris’ approval for NMOSD was based mainly on data from a global, placebo-controlled Phase 3 trial called PREVENT (NCT01892345).
PREVENT
The PREVENT study enrolled 143 adults with NMOSD and anti-AQP4 antibodies across 18 countries, including the U.S. Eligible patients had experienced at least two relapses in the prior year, or three relapses in the previous two years with at least one having occurred in the past year.
Participants were randomly assigned to receive either Soliris or a placebo according to the now-approved dosing regimen. Treatment was slated to be given until 24 patients had experienced a relapse as adjudicated by an independent panel. Patients on stable-dose immunosuppressive therapies, except rituximab, were allowed to continue such treatment.
Ultimately, the trial was ended after just 23 patients — and not 24 — experienced an adjudicated relapse; it was unclear how much longer it would be until the final event occurred.
The results showed that the therapy significantly reduced the relapse risk by 94%, with adjudicated relapses being reported in 3% of the Soliris-treated patients. That compared with adjudicated relapses in 43% of individuals in the placebo group.
Overall, Soliris was found to result in a significantly lower annualized relapse rate, of 0.02 versus 0.35 relapses per year, compared with the placebo.
More than 96% of patients treated with Soliris remained relapse-free after more than 2.5 years. In comparison, during that same time period, fewer than half of the patients on the placebo (45.4%) did not experience a relapse.
Data from individuals who were not receiving other immunosuppressive treatments also favored Soliris, with none of the patients on the therapy experiencing an adjudicated relapse, compared with 54% of patients on a placebo.
Soliris also tended to be superior to the placebo at slowing disability progression and improving quality of life, but these differences failed to reach statistical significance.
Open-label extension
After completing the trial, a total of 119 patients chose to join an open-label extension study (NCT02003144), in which all received Soliris for up to 6.5 years.
Combined data from PREVENT and its extension showed that Soliris continued to reduce the risk of relapse. Indeed, 93.9% of patients in the extension trial remained relapse-free after more than 3.5 years from the start of PREVENT.
Researchers noted that this proportion was even greater (96.2%) among patients receiving Soliris without other immunosuppressive medications.
Ongoing trials
Soliris now is being tested in 12 children and adolescents with AQP4-related NMOSD as part of an international Phase 3 trial (NCT04155424).
The participants, ages 2-17, are receiving weight-based doses of Soliris in a similar pattern to adults in the trial. Specifically, the children receive five weekly loading doses followed by every-other-week maintenance doses.
Treatment will be given for about one year, after which participants will have the option to continue Soliris during an extension period of about two years.
The study’s main goal is to assess changes in relapse rate and time to first relapse. Secondary measures include changes in disability levels, quality of life, vision, and blood levels of Soliris and C5 protein. The trial is set to end by mid-2025.
Common side effects of Soliris
The most common side effects of Soliris in NMOSD clinical trials include:
- upper respiratory infection
- common cold
- diarrhea
- back pain
- dizziness
- flu (influenza)
- joint pain
- sore throat
- bruising.
Infections
Soliris carries a boxed warning for an increased risk of serious meningococcal infections while on the therapy. These infections can rapidly become life-threatening or fatal if not detected and treated early.
Patients starting on Soliris should complete or update their meningococcal vaccination at least two weeks before the first dose of the therapy, according to current vaccination guidelines for patients on complement-blocking therapies. If the risks of delaying treatment outweigh the potential risks of serious meningococcal infections, an unvaccinated individual may start the therapy. However, any such patients should receive the vaccine as soon as possible, along with two weeks of preventive antibacterial treatment.
Patients and their physicians should discuss the benefits and risks of Soliris treatment, as well as of preventive antibacterial treatment in unvaccinated or vaccinated patients, against the known risks for serious meningococcal infections.
Given such vaccines reduce, but not completely eliminate, the risk of meningococcal infections, patients should be routinely monitored for early signs of these infections. These may include headache, stiff neck, fever, confusion, nausea and vomiting, and photophobia, in which the eyes are more sensitive to light. If a meningococcal infection is suspected, patients should be immediately evaluated, and treated if such infection is confirmed. Soliris may be discontinued if treatment for serious meningococcal infections is needed, depending on the risks of interrupting treatment.
Because Soliris works by reducing immune activity, patients on the therapy also may have an increased risk of other types of infections, especially those from bacteria that are normally fought off by the complement cascade. Caution is recommended when administering the therapy to people with any whole-body infection.
Infusion-related reactions
Soliris can cause infusion-related reactions, including allergic reactions that can be serious and life-threatening. Still, no treatment discontinuation due to infusion-related reactions were reported in Soliris trials. If patients show signs of cardiovascular or respiratory problems, Soliris infusion should be interrupted and appropriate supportive measures should be given, as needed.
Use in pregnancy and breastfeeding
There are limited data regarding Soliris’ effects on pregnancy outcomes and on breastfed infants.
While animal findings suggest that C5-targeting antibodies like Soliris may cause damage to the developing fetus, data from more than 300 women on Soliris during pregnancy suggested no safety issues. Also, Soliris’ presence in human breast milk has not been rigorously studied, and its potential effects on nursing infants and on milk production in nursing patients remain unclear.
Patients who are pregnant or nursing, or plan to become pregnant or breastfeed, should discuss this topic with their healthcare team and carefully weigh the potential benefits and risks of using Soliris in these circumstances.
Neuromyelitis News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
FAQs about Soliris
Category:
Soliris
There is no known interaction between alcohol and Soliris. However, because alcohol can interfere with some medications, it is recommended that patients talk about this issue with their healthcare providers.
Category:
Soliris
Animal studies have suggested that anti-C5 antibodies such as Soliris can cause fetal harm, but data from more than 300 women exposed to Soliris during pregnancy raised no safety concerns. Still, it remains unclear if Soliris can result in harm to a developing human fetus, so patients who become or plan to become pregnant while on the medication should discuss this topic with their physician.
Category:
Soliris
Weight gain has not been reported as a side effect of Soliris in clinical trials of people with neuromyelitis optica spectrum disorder. However, some trial participants given Soliris experienced reduced appetite and hair loss, and at a higher proportion than that observed in the placebo group. Patients should speak with their healthcare provider if they experience any unanticipated side effects with Soliris.
Category:
Soliris
In the PREVENT trial, which supported Soliris’ approval for neuromyelitis optica spectrum disorder (NMOSD), significant differences in the proportion of relapse-free patients between the treatment and placebo groups were already evident after about 48 weeks, or nearly one year. However, each patient is unique and may respond differently to the medication; thus, individuals with NMOSD are advised to talk with their healthcare team to better understand how Soliris may help in their specific case.
Category:
Soliris
The U.S. Food and Drug Administration (FDA) approved Soliris in June 2019 for adults with neuromyelitis optica spectrum disorder who are positive for antibodies against the AQP4 protein. That decision marked the first FDA approval of a treatment for this rare autoimmune disease.
Related Articles
-
-
 Discussion
Discussion
-
-
 Discussion
Discussion
-

-
Discussion